
Beyond the Eye -Why Estimating Body Blood Volume is Critical in PPH?
In the management of Postpartum Hemorrhage (PPH), clinicians often focus on the volume of blood on the floor. However, the most critical number isn’t just what was visibly lost—it’s what remains. Estimating a patient’s baseline body blood volume is the only way to understand the true physiological impact of a hemorrhage.
Scope of Discussion
This article revisits the limitations of relying solely on visual estimation and fixed numerical thresholds when assessing postpartum blood loss.
It does not discuss detailed postpartum haemorrhage management or transfusion protocols. The aim is to refine how blood loss is interpreted in day-to-day clinical practice.
The Problem with a “One Size Fits All” Approach
In obstetrics, clinicians are familiar with thresholds such as:
- 500 mL for postpartum haemorrhage after vaginal delivery
- 1.5 L for massive postpartum haemorrhage
These are important clinical references. However, they are sometimes applied too rigidly, as though every patient has the same physiological reserve.
In reality, these thresholds are based on a “ideal patient” and should not replace individual clinical assessment.
Why Estimated Blood Volume Matters
Traditionally, clinicians estimate maternal blood volume using a simple linear formula based on body weight. However, newer evidence suggests this may oversimplify the relationship between body size and circulating blood volume, particularly at extremes of body mass.
Current evidence suggests circulating blood volume does not increase proportionally with body weight, especially in obesity.(1)
A small-built patient may therefore tolerate blood loss very differently compared to a larger patient, while in obesity, relying purely on body weight may result in overestimate physiological reserve.
This becomes even more important in patients who already begin labour with borderline haemoglobin levels.
How to Estimate Body Blood Volume and % Loss
1. Calculate the Baseline: Consider the patient’s weight and BMI when estimating total body blood volume, as evidence shows it does not increase proportionally with weight, especially in obesity. (1) Use the following table to aid calculation.
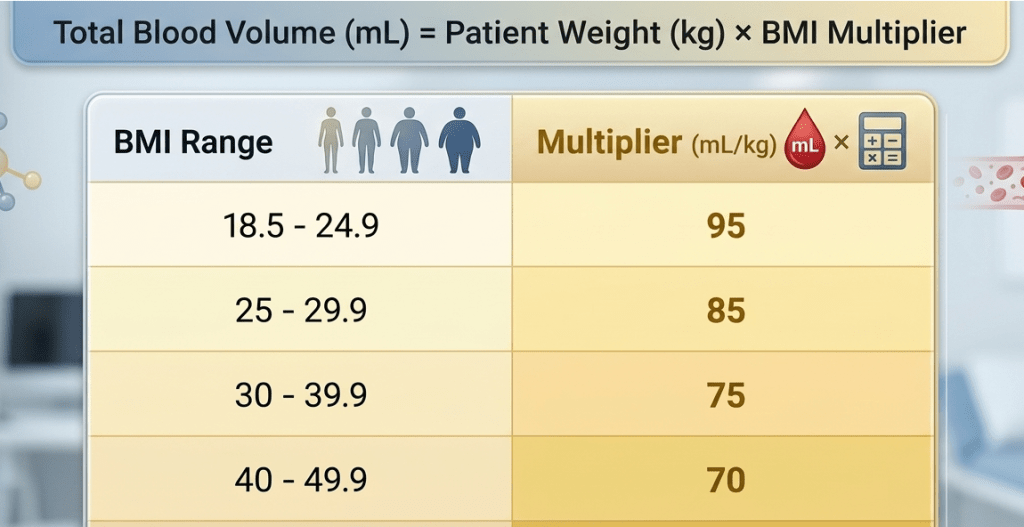
Table reference (1) .
For example at 96kg patient with BMI of 40kg/m2 will have an estimated TBV of 6.7ltr (96kg X 70ml/kg) i.e patient’s weight (kg) X the multiplier for the corresponding BMI.
2. Identify the “Percent Loss”:

Looking Beyond the Number
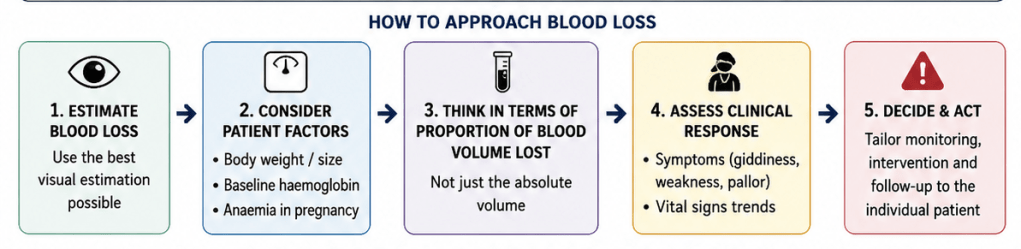
Blood loss assessment should not stop at estimating volume alone. Clinical interpretation should also consider:
- Baseline haemoglobin.
- Symptoms such as giddiness or weakness.
- Physiological response over time
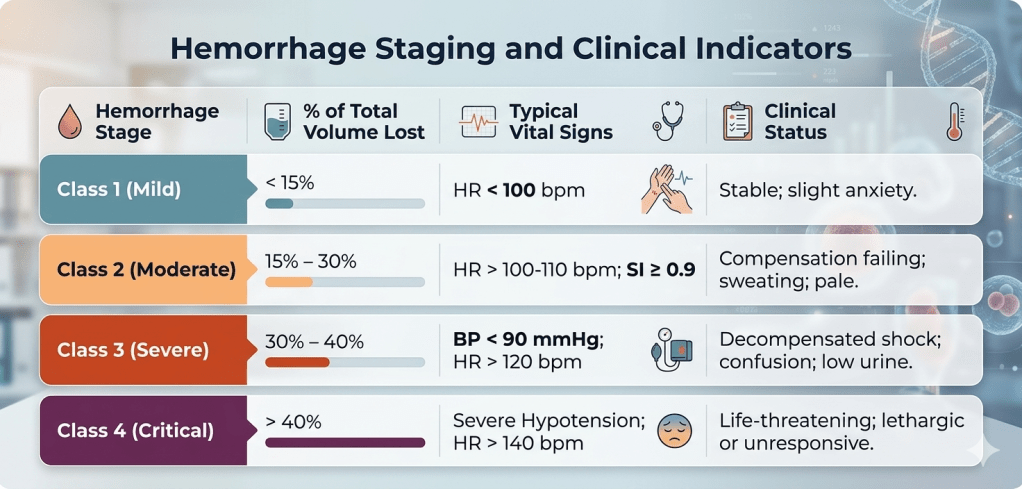
Haemorrhage Staging and Clinical Indicators (table above) are vital for spotting patients at risk, even when visible blood loss or estimated blood volume loss seems acceptable. This thorough evaluation enhances patient safety and supports timely medical actions, highlighting the importance of looking beyond just numbers.
Final Takeaway
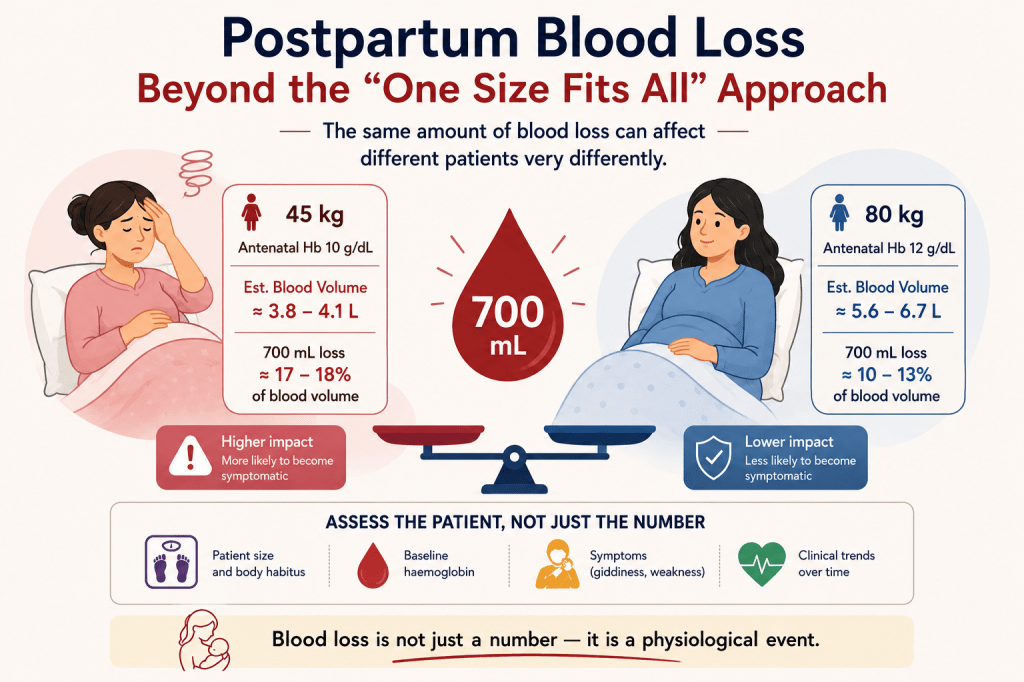
Blood loss is not just a number — it is a physiological event.
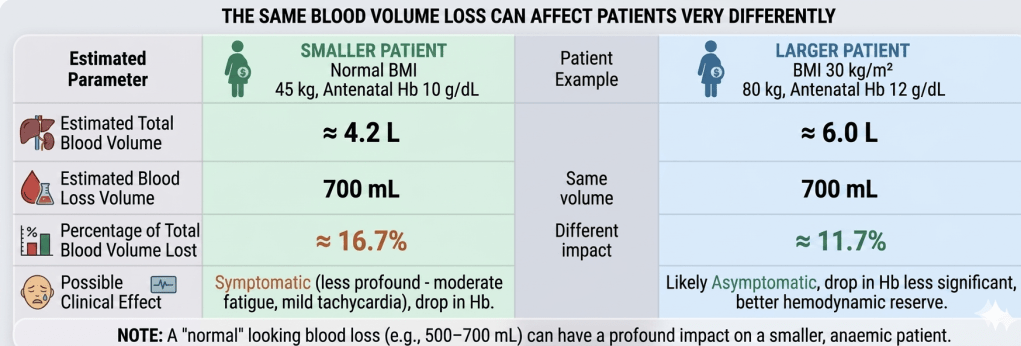
The same amount of blood loss can affect different patients very differently.
Ref:
1. Kennedy H, Haynes S, Shelton C. Maternal body weight and estimated circulating blood volume: a review and practical nonlinear approach. British Journal of Anaesthesia, 2022; 129, 716-725
This series aims to support practical refinements in everyday obstetric care across hospitals, health clinics, and MCHCs. Future topic suggestions, feedback, and clinical questions are welcome. Leave it in the comment below.
Written by:
Dr Nuruhuda bt Samsudin
Obstetrician & Gynaecologist
Sarawak General Hospital

Leave a comment