
Caesarean Wound Breakdown: When Secondary Healing Is Enough
Wound breakdown following caesarean section is not uncommon. It often presents after discharge, when follow-up takes place in hospitals, health clinics, or MCHCs.
A familiar pathway is often followed i.e. the wound opens, dressings are started, and a plan is made for re-closure.
However, not every wound requires surgical closure. In some cases, the wound is already progressing well with secondary intention healing, and intervention may not improve the outcome.
This article revisits a simple but important question:
when is closure necessary, and when is it not?
Scope of Discussion
This discussion focuses on decision-making after caesarean wound breakdown, particularly the choice between continuing secondary intention healing and proceeding to delayed primary closure.
It does not cover prevention, dressing techniques, antibiotic use, or management of deep fascial dehiscence. The emphasis here is on recognising wound progress and deciding whether intervention is required.
Starting with the Basics
Assessment should include the extent of separation, presence of infection, and the condition of the wound bed. Most importantly, the integrity of the rectus fascia must be confirmed.
If there is concern about fascial involvement, urgent surgical review is required. This discussion applies only to superficial wound breakdown with intact rectus fascia.
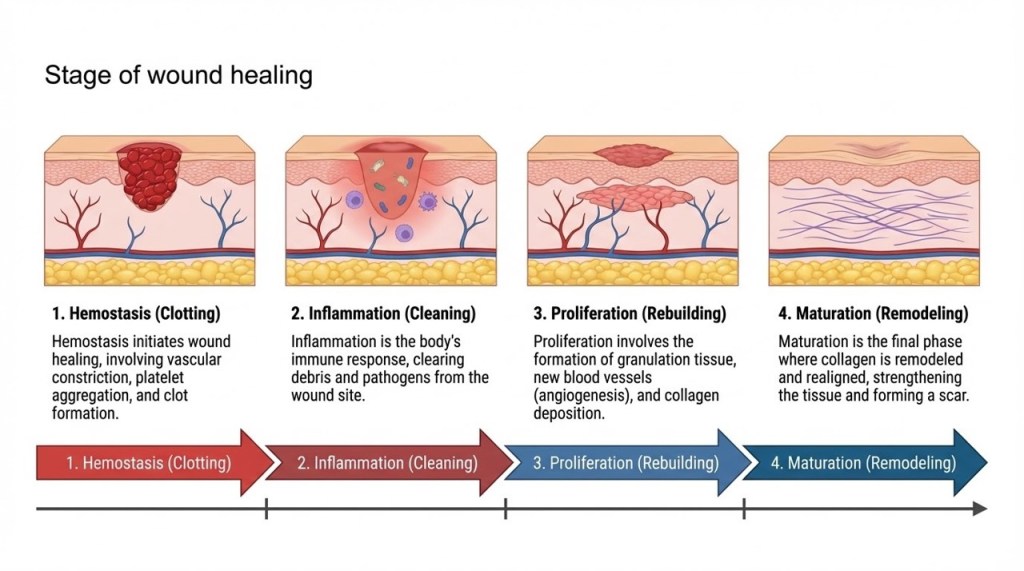
Understanding Secondary Intention Healing
Secondary intention healing is not merely a temporary step. It is a natural and effective healing process.
As infection settles, granulation tissue forms and the wound begins to contract progressively. This progression indicates that healing is underway.
This is appropriate when:
- There is active infection
- The wound contains slough or non-viable tissue
- The wound requires ongoing drainage
- The wound edges are not suitable for closure
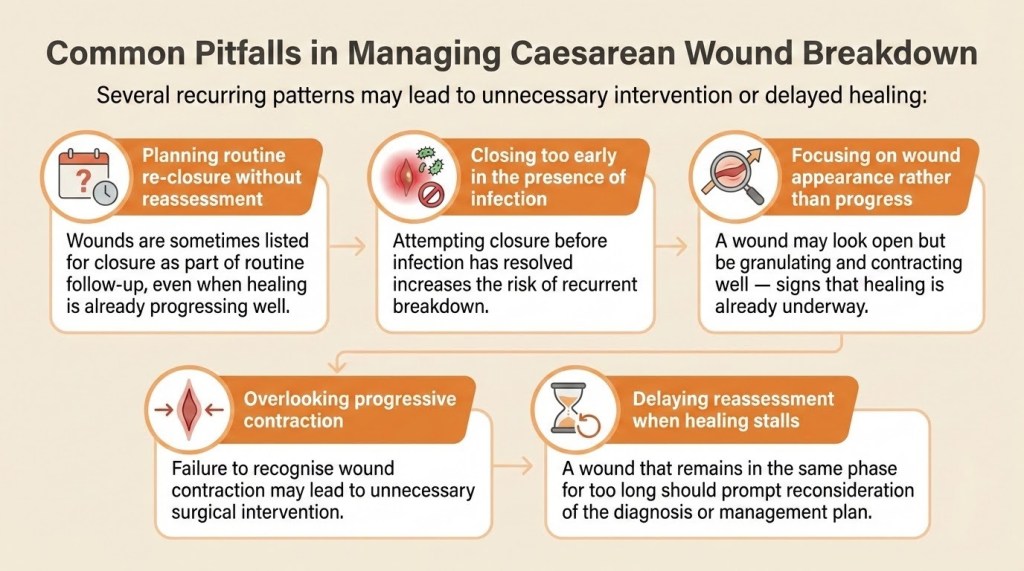
Attempting closure too early, especially in the presence of infection, risks further breakdown.

When to Consider Closure
Delayed primary closure may be considered once the wound is clean, infection has resolved, wound can be oppose without tension and healthy granulation tissue is present.
While closure may shorten healing time, it should be selective rather than routine.
When Secondary Healing Is Enough
In practice, some wounds progress well once secondary intention healing has been established.

- Healthy granulation tissue present
- Wound progressively contracting
- No ongoing infection
- Wound size is reducing over time
At this stage, it is not uncommon for patients to be scheduled for re-closure as part of routine planning. Yet in many of these cases, the wound is already on a clear path to healing.
Continuing conservative management may be entirely appropriate, especially if the wound is reducing in size and the patient is coping well with dressings. Surgical closure in such situations may offer only limited additional benefit.
Practice Principle
A wound that is healing well by secondary intention does not always need to be closed.
Recognising When to Reassess
Wound healing should show steady progression. When this progression is not seen, it is important to pause and reassess.
A wound that remains in the same phase for a prolonged period, shows poor granulation, or has persistent discharge may indicate underlying issues. These could include ongoing infection, suboptimal wound care, or patient-related factors affecting healing.
In such situations, early input from a wound care team or senior clinician can be helpful.
Quick Reminder
Good wound management is guided by progress, not appearance.
A Practical Perspective
In everyday practice, the decision to close a wound should not be routine. It should be based on how the wound is behaving.
A clean, well-granulating wound that is progressively contracting is already healing. In many cases, allowing this process to continue is sufficient.
Final Takeaway
The objective is wound healing — not necessarily wound closure.
This series supports practical refinements in everyday obstetric care across hospitals, health clinics, and MCHCs.
Future topic suggestions, feedback, and clinical questions are welcome.
Written by:
Dr Nurulhuda binti Samsudin
Obstetrician & Gynaecologist
Sarawak General Hospital

Leave a comment