
Among the challenges in the management of anemia in pregnancy is the number of possible differential diagnosis for the underlying cause. This ranges from the haemodilutional effect of physiological plasma expansion in pregnancy to iron deficiency anaemia (IDA), and less common causes such as haemoglobinopathy.
To complicate matters, these conditions may occur concurrently in the same antenatal patient.
Getting the correct diagnosis allows for effective and safe management of anaemia.
This article focuses on how serum ferritin (Se ferritin) can help clinicians achieve this in day-to-day practice, particularly in the Maternal and Child Health Clinic (MCHC) setting.
Scope of Discussion
This article does not discuss in detail the full investigation and management of anaemia in pregnancy.
Its aim is to refine day-to-day clinical practice in the diagnosis and management of anaemia using Se ferritin, and to revisit some basic principles.
The practical application of this article may be limited by the availability of Se ferritin testing. Where this investigation is not available, alternative diagnostic approaches are not discussed here.
A Simple Introduction to Ferritin
Ferritin is a major iron storage protein that also plays an important role in iron regulation in the human body.
Low ferritin therefore indicates reduced iron stores, and the patient is at risk of iron deficiency anaemia. Conversely, high ferritin may indicate iron overload.
However, it is important to note that inflammatory conditions can also increase serum ferritin levels.
A serum ferritin level <30 ng/mL is generally accepted as diagnostic of iron deficiency anaemia, with good sensitivity, bearing in mind that ferritin may be elevated in inflammatory states.
Investigating Anaemia in Pregnancy – Getting the Basics Right
The initial investigations for anaemia in pregnancy include:
- Full blood count (FBC)
- Peripheral blood film (PBF)
- Iron studies (this usually includes Se Ferritin where available)
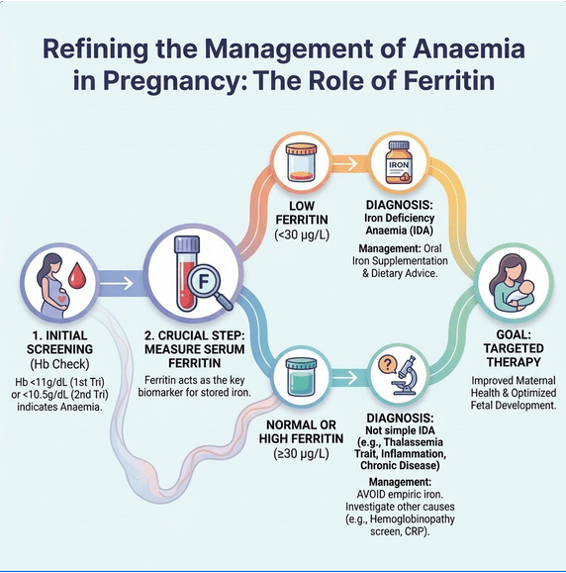
Following the diagnosis of IDA, start oral iron elemental dose of 60 to 120 mg daily. Hb is repeated in 2-4 weeks to monitor response and the expected response is at least 1g/dl after 2 weeks. Once Hb normalize (⩾11g/dl), the oral iron dose can be reduce to 30-60mg daily.
The peripheral blood film is particularly useful in screening for haemoglobinopathies such as thalassaemia, especially in patients with anaemia but normal Se ferritin, or when iron deficiency anaemia does not respond to iron therapy.
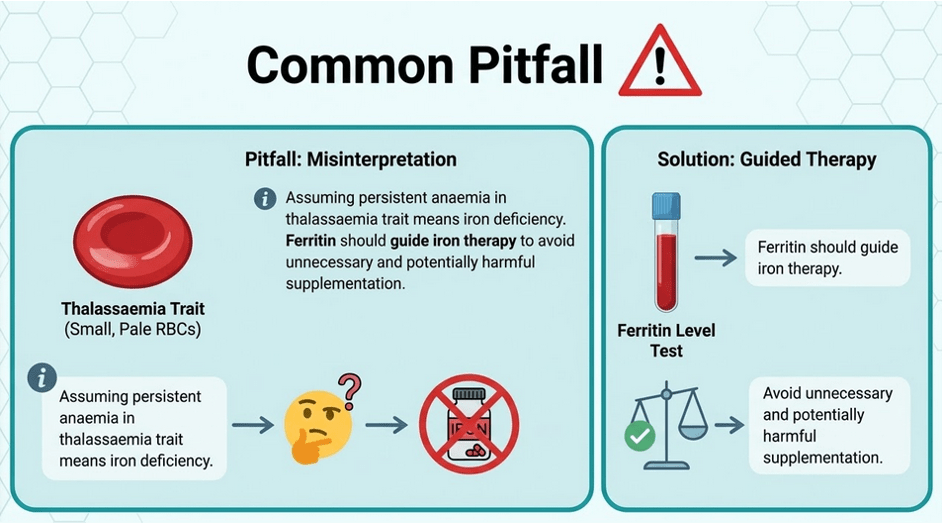
Ferritin therefore plays an important role not only in diagnosing iron deficiency, but also in guiding safe iron supplementation in pregnancy.
This is particularly relevant in Malaysia where thalassaemia trait is common, as unnecessary iron therapy may lead to inappropriate treatment while the underlying cause of anaemia remains unrecognised.
Safe Iron Supplementation in Pregnant Women with Mild Haemoglobinopathy (e.g. Thalassaemia Trait) – Role of Se Ferritin
Pregnant women with thalassaemia trait and concurrent iron deficiency anaemia will benefit from oral iron supplementation. Se ferritin levels help identify these patients.
Following iron supplementation, Se ferritin should be monitored at 2–3 monthly intervals to evaluate response.
Haemoglobin alone may not be a reliable guide, as patients may remain anaemic due to the underlying haemoglobinopathy.
Oral iron supplementation should be discontinued once ferritin levels normalise, a reasonable target value would be 40 – 50 mcg/L. Monitoring can continue with both haemoglobin and Se ferritin after that.
Final Takeaway:
Ferritin helps move the diagnosis from assumption to confirmation.
This series aims to support practical refinements in everyday obstetric care across hospitals, health clinics, and MCHCs.
Leave a comment below for future topic suggestions, feedback, and clinical questions. Shared experiences often highlight areas where further discussion may benefit clinical practice.
Reference:
Ubom AE, Begum F, Ramasauskaite D, et al. FIGO good practice recommendations on anemia in pregnancy, to reduce the incidence and impact of postpartum hemorrhage (PPH). Int J Gynecol Obstet. 2025;171:993-1007. doi:10.1002/ijgo.70529
Written by;
Dr Nurulhuda bt Samsudin
Obstetrician & Gynaecolgist
Sarawak General Hospital

Leave a comment